Types of Connective Tissues :

Type # 1. Loose Connective Tissue:
(A) Areolar Tissue (= Loose connective tissue):
This tissue is most widely distributed connective tissue in the animal body.
Structure:
Structure:
It is named so because it takes the form of fine threads crossing each other in every direction leaving small spaces called areolae.
The areolar tissue consists of ground substance, the matrix, white, yellow and reticular fibres and cells like fibroblasts, mast cells, macrophages (= histocytes or clasmatocytes), lymphocytes, plasma cells, mesenchyme cells, chromatophores.
Fat cells can be seen in small groups. Description of matrix, fibres and cells has already been given in the general structure of connective tissue.
Location:
Location:
As stated earlier, the areolar tissue is the most widely distributed connective tissue in the body. It is present under the skin as subcutaneous tissue in between and around muscles, nerves and blood vessels in sub-mucosa of gastrointestinal tract and respiratory tract, in the bone marrow, between the lobes and lobules of compound glands and in mesenteries and omenta.
It also forms the internal frame work (= stroma) of many solid organs. In fact it forms packing nearly in all organs.


Functions:
To bind parts together is the primary function of areolar tissue. Other functions are to provide strength, elasticity, support to the parts where this tissue is present. It also provides rapid diffusion of materials and migration of wandering cells towards areas of infection and repair.
(B) Adipose Tissue:
It is a fat storing connective tissue.
Structure:
The adipose tissue consists of several spherical or oval adipose cells (= adipocytes or fat cells; Fig. 7.16). Each adipose cell contains fat globules, due to which the nucleus and the cytoplasm are displaced to the periphery.These cells are often called signet ring cells because they resemble a signet rang when seen in cross section. There are two types of adipose tissue: white (or yellow) fat and brown fat. White fat contains large adipose cells, each having a single large fat globule and hence, called monolocular.

The cytoplasm in these cells is pushed to a peripheral layer containing nucleus. The adipose cells of brown fat are multilocular, each cell with several small fat globules. Brown colour is due to iron containing cytochrome pigment in fat.
Brown fat found in those mammals which have an oxidation power 20 times more than that of yellow fat because brown fat cells are loaded with a large number of mitochondria.
Brown fat is found in hibernating mammals such as rats and other rodents and in new-born human babies. The fibres are few in number and form a loose network for supporting the fat-laden cells. If these cells are treated with alcohol, the fatty substance is dissolved and the cells become vacuolated.
Location:
The adipose tissues are found in the subcutaneous tissue, around the heart, kidneys, eyeballs, mesenteries and omenta, where fat is stored. Adipose tissue is also found in the blubber of whales and elephants, hump of camel, fat bodies of frog and yellow bone marrow.
Functions:
The adipose tissue is chiefly a food reserve or ‘fat depot’ for storage. The sub cutaneous fat prevents heat loss from the body and also rounds off the body contour.
It forms a shock-absorbing cushion around the eye balls and kidneys. It also provides support and protection. This tissue also helps in the production of blood corpuscles. We become fatty when our body cells accumulate fat globules. Excessive accumulation of fat is called adiposis.
Type # 2. Dense Connective Tissue:
It is of two types; dense regular connective tissue and dense irregular connective tissue.
(A) Dense Regular Connective Tissue:
In the dense regular connective tissue, the collagen fibres are present in rows between many parallel bundles of fibres. It is also of two types: white fibrous connective tissue and yellow elastic connective tissue.
1. White Fibrous Connective Tissue:
It consists of mainly white (collagen) fibres which are arranged in bundles. The fibroblasts are present in rows between the bundles.
(i) White Fibrous Cords (Tendons):
The white fibrous connective tissue forms cords called tendons which connect the skeletal muscles with the bones.
(ii) White Fibrous Sheets:
White fibrous connective tissue also forms flat plates or sheets. It occurs in the dermis of the skin, connective tissue sheaths of muscles and nerves and tunica adventitia (= outer coat) of large blood vessel, periosteum of the bone, perichondrium of the cartilage, pericardium of the heart, diameter of the brain and spinal cord, renal capsule of the kidney, sclera and cornea of the eye ball and fibrous capsules of penis and testes and between skull bones.
White fibrous connective tissue has great strength, however, its flexibility is limited. The presence of white fibrous tissue at the joints between skull bones makes them immovable. Due to presence of abundant white fibres, the skin dermis of large mammals yields leather after chemical treatment called tanning.

2. Yellow Elastic Connective Tissue:
This tissue is mainly made up of much thicker branched loose network of yellow fibres. The white fibres also occur but they are very fine. The fibroblasts are irregularly scattered. It also contains mast cells, macrophages and often some adipose cells.
(i) Yellow Fibrous Cords (Ligaments):
The yellow elastic connective tissue forms cords called ligaments which join bones to bones.
(ii) Yellow Fibrous Sheets:
The sheets formed by this tissue occur in the walls of blood vessels, lungs, bronchioles, true vocal cords, cartilage of larynx, trachea, capsules of spleen and ligamenta flava which connect adjacent vertebrate.
Yellow Elastic Connective tissue has considerable strength and remarkable elasticity.
Thus it allows stretching of various organs.
Many years old ‘mummies’ still have their arteries intact due to well preserved elastic fibres.
Sprain is caused by excessive pulling (stretching) of ligaments.
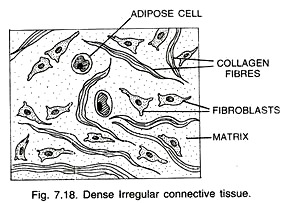
(B) Dense Irregular Connective Tissue:
It has fibroblasts and many fibres (mostly collagen) that are oriented differently. This tissue is present in the skin.
Type # 3. Specialised Connective Tissues:
These are of the following types:
(A) Skeletal Tissues:
These connective tissues form the endoskeleton of the vertebrates. Hard parts of the body constitute skeleton. These support the body, protect the various organs and help in locomotion. Skeletal tissues include cartilage and bone.
1. Cartilage (= Gristle):
Cartilage is a soft skeletal tissue. It is not rigid like bone. It is found more abundantly in vertebrate embryos because most of the bones forming skeleton of the adult are cartilaginous in the early stage. However, it is commonly found in the body of adult vertebrates.
Structure of Cartilage:
A typical (generalized) cartilage consists of the following parts:
(i) Cartilage Cells:
A cartilage cell is present in a fluid filled space, the cartilage lacuna (pi. lacunae), which affects the shape of the cell. Young cartilage cells are relatively small, often flattened with many small surface projections (filopodia) and are called chondroblasts (this term is also used for embryonic cartilage producing cells).
Mature cells are larger in size (these cells increase in size with age), more rounded, but still have a few surface projections and are known as chondrocyres. The chondrocytes are metabolically more active cells than chondrocytes.
(ii) Ground Substance (= Matrix):
It consists essentially of water, proteoglycans (proteins and carbohydrates), some lipid, collagen, non-collagenous protein, and collagen fibres. The core protein (mucoprotein) is aggrecan.
The carbohydrates are chemically glycosaminoglycan’s (GAG). They include chondroitin sulphate, keratin sulphate and hyaluronic acid. Keratin sulphate increases with maturity. These molecules form a firm gel that gives firm consistency to the ground substance of the cartilage.
A gelatin-like substance obtained from cartilage by boiling is called chondrin. The free surfaces of hyaline cartilage (to be described ahead) are covered by a fibrous membrane called the perichondrium but it is not present in fibrous cartilage. The perichondrium contains blood vessels.
Cartilage is usually described as an avascular (without blood supply) tissue but it is not true. There are present cartilage canals, through which blood vessels may enter cartilage.
Cartilage cells receive their nutrition by diffusion from blood vessels in the perichondrium or in cartilage canals. Cartilage canals may play a role in the ossification (formation of bones) of cartilage by carrying bone forming cells. The growth of the cartilage is always from the periphery (unidirectional).
Types of Cartilages:
The cartilages are of three types:
(a) Hyaline Cartilage (hyalos = glass’, Fig. 7.19):
It contains clear, large amount of translucent, slightly elastic matrix with less fibres. The matrix often has very fine white fibres which are difficult to observe. It is most prevalent cartilage. It forms articular surfaces at the joints of long bones, where it is called articular cartilage.
It forms rings of trachea and bronchi, sternal parts of ribs (= costal cartilages), hyoid apparatus, nasal septum and also part of larynx. Most of the embryonic skeleton consists of hyaline cartilage. Hyaline cartilage forms the skeleton of elasmobranch fishes (cartilaginous fishes) and the embryonic skeleton in bony vertebrates.

(b) Fibrous Cartilage:
It has well developed fibres in the matrix. It is of two types: White fibrous cartilage and yellow elastic fibrocartilage.
(i) White Fibrous Cartilage or White Fibrocartilage:
The matrix is firm and has abundant white fibres. It occurs in the intervertebral discs where it acts as cushion and in the pubic symphysis (region between the two pubic bones of the pelvic girdle) where it helps in parturition (process of birth). White fibrous cartilage is the strongest cartilage (Fig. 7.20).

(ii) Yellow Elastic Fibrocartilage (Fig. 7.21):
The matrix contains numerous yellow fibres which form a network by uniting with one another. Due to the presence of yellow fibres, the cartilage becomes more flexible. This type of cartilage is found in the pinna and external auditory canal of the ear, Eustachian tubes, epiglottis and tip of the nose. It makes these organs flexible.

(c) Calcified Cartilage:
Sometimes matrix contains granules of calcium carbonate, then the cartilage is called calcified cartilage. Calcium carbonate makes the cartilage hard and inelastic. This cartilage is found in supra scapula of pectoral girdle of frog and vertebrae of shark.

2. Bone:
Bone is the hardest tissue in the body and supports various organs. The matrix is tough containing both inorganic and organic substances. The inorganic salts present in the matrix are calcium phosphate, calcium carbonate, calcium fluoride, magnesium phosphate, etc.
If a bone is dried, its organic matter (living matter) is destroyed and inorganic part is left behind. On the other hand if a bone is kept in a dilute HCL for some time, its inorganic part is dissolved and organic part is left behind.
Such a bone is called decalcified bone. Study of a dried bone shows its inorganic matter, while that of a decalcified bone reveals the animal matter. Thus bone may be studied in two forms: decalcified and dried.
Microscopic Structure of Decalcified Mammalian Bone:
It consists of four parts: periosteum, matrix, endosteum and bone marrow.
(a) Periosteum:
It is a thick and tough sheath that forms an envelope around the bone. It is composed of collagen (= white) fibrous tissue. Bundles of periosteal collagen fibres, called Sharpey’s fibres, penetrate the bone matrix to provide a firm connection between the two. The periosteum contains blood vessels. The periosteum also contains bone-forming cells, the osteoblasts which produce new bone material.

(b) Matrix:
It is composed of a protein called ossein. The main salts found in the matrix are calcium phosphate, calcium carbonate, sodium chloride and magnesium phosphate. Of these calcium phosphate is maximum in the vertebrate bone.
The Haversian canals, a characteristic feature of the mammalian bones, are present in the matrix. Each Haversian canal contains an artery, a vein, a lymph vessel, a nerve and some bone cells, all packed in with connective tissue. The Haversian canals are interconnected by transverse channels, the Volkmann’s canals.

The matrix has numerous inactive bone cells, the osteocytes. The latter contain reduced numbers of cell organelles and often store glycogen. An osteocyte is surrounded by a fluid-filled space, the bone lacuna, which leads into fine radiating channels, the canaliculi (minute canals).
In the developing bone, the osteocytes give off several projections called protoplasmic processes (= filopodia) which extend through the canaliculi. With the help of canaliculi and protoplasmic processes one osteocyte is in contact with another osteocyte. The matrix of the bone occurs as layers called lamellae.
The lamellae are of four types:
(a) Haversian lamellae:
These lamellae occur around the Haversian canals. A Haversian canal with its surrounding lamellae and osteocytes constitute a cylindrical unit of bone called Haversian system or osteon.
Haversian systems are absent in spongy bones of mammals:
(b) Interstitial lamellae:
These lamellae occur between the Haversian systems,
(c) Outer circumferential lamellae (= outer concentric lamellae):
These lamellae occur inner to periosteum,
(d) Inner circumferential lamellae (= inner concentric lamellae):
These lamellae occur outer to endosteum.
(c) Endosteum:
It is present outer to the bone marrow cavity. Like the periosteum, it comprises white fibrous tissue and osteoblasts (bone forming cells). But the white fibrous tissue is present here inner to osteoblasts. The long bone thus grows in thickness from two sides. This type of growth is called bidirectional growth.
(d) Bone Marrow:
In long bones such as limb bones (humerus, femur, etc.) a cavity called bone marrow cavity is present inner to the endosteum. The bone marrow cavity is filled with a soft and semisolid fatty neurovascular tissue termed as bone marrow. In fact bone marrow is a special kind of tissue which is called myelogenous or myeloid tissue.

Types of Bone Marrow:
It is of two types:
(a) Red bone marrow:
It is red due to abundant blood vessels. It is present in the spongy parts of the bones (e.g., epiphyses). It produces red blood corpuscles, white blood corpuscles (monocytes, eosinophil’ss, basophils and neutrophils) and platelets,
(b) Yellow bone marrow:
It is present in the shafts of long bones. It is yellow in colour and has much fatty tissue. It produces blood corpuscles in emergency, i.e., at the time of excessive loss of blood; when it changes into red bone marrow.
During foetal life and at birth there is red bone marrow throughout the skeleton. After about the fifth year the red bone marrow is gradually replaced in the long bones by yellow bone marrow.
By 20 to 25 years the red bone marrow persists only in the vertebrae, sternum, ribs, clavicles, scapulae, pelvis, cranial bones and in the proximal ends of femora (pi. of femur) and humeri (pi. of humerus). In old age the bone marrow of the cranial bones undergo degeneration and is then called gelatinous marrow.
Types of Bone:
On the basis of its texture, a bone is of two types: compact and spongy (cancellate).
(i) Compact (Dense) Bone:
It is comparatively hard and compact. It is found in the shaft of long bones. It contains yellow bone marrow and has Haversian systems.
(ii) Spongy (Cancellate) Bone:
It consists of a network of thin and irregularly longitudinal and tranverse bony bars called trabeculae covered by the endosteum. It is found at the ends of long bones (epiphyses). Spongy bone contains red bone marrow but it is without Haversian systems.
Types of Bones:
According to their source of formation.
(i) Cartilaginous or Replacing Bones:
These bones develop from the pre-existing cartilage and practically replace the cartilage. Examples: humerus, femur.
(ii) Investing or Dermal or Membrane Bones:
These bones develop in the dermis of the skin as thin plates and sink to get attached over the original cartilaginous endoskeleton. In fact these bones become invested upon original cartilages hence their name. Examples: frontal, nasals, vomers and parietals of the skull.
(iii) Sesamoid Bones:
These bones are formed in the tendons at the joints. Example: patella (knee-cap).
(iv) Visceral Bones:
These are formed in the soft organs (= viscera). Examples: os cordis in the heart of some ruminants (e.g., deer), os penis in the penis of most bats, insectivores, rodents (e.g., rats), carnivores (e.g., dog, walrus), whales, some primates (not man), os clitoris in the clitoris of many carnivores, and os palpebrae in the eyelids of crocodiles.
A small bone also develops in the crest of a bird and snout of a hog. Bone acts as a reservoir for ion like calcium, magnesium and phosphorus.
(B) Vascular Tissues (= Fluid Tissues):
Vascular tissues are motile connective tissues consisting of fluid matrix and free cells. The matrix is without fibres. The matrix is not secreted by the cells present in it. Vascular tissues transport the materials from one place to the other.
Types:
The vascular tissues are of two types: blood and lymph.

I. Blood:
Blood is a mobile connective tissue composed of a fluid, the plasma and the cells, the blood corpuscles. Blood is basis of life. Blood is the softest tissues in the body.
Fluids outside the cells are generally called extracellular fluids (ECF). Blood forms about 30-35 percent of the ECF. The volume of blood in an adult person of 70 kg weight is about 5.5 litres. It is a slightly alkaline fluid having pH 7.4. pH of blood in arteries is more than in veins.
Composition:
As stated above blood is composed of a watery fluid called plasma and floating bodies termed formed elements {e.g., blood corpuscles).
(A) Plasma:
It is slightly alkaline non-living intercellular substance which constitutes about 55% part of the blood. It is a pale yellow but transparent and clear fluid.
Composition of Plasma:
1. Water:
Water alone forms about 90% to 92% of the plasma. Solids form about 8% of the plasma.
2. Mineral Salts:
These are chlorides, bicarbonates, sulphates and phosphates of sodium, potassium, calcium, iron and magnesium. All salts constitute about 0.9% of plasma. Buffer of the blood is sodium bicarbonate.
3. Nutrients:
These include glucose, fatty acids, phospholipids, cholesterol, fats, amino acids, nucleosides, etc. Mineral salts have been mentioned above.
4. Plasma Proteins:
They constitute about 7 to 8% part of plasma. These mainly include albumin, globulin, immunoglobulin, prothrombin and fibrinogen.
5. Defence Compounds:
Immunoglobulin’s which act as antibodies and some other substances, such as lysozyme (a polysaccharide) and properdin (a large protein) are always found in the plasma. They destroy bacteria, viruses and toxic substances that may enter into the blood from outside.
6. Excretory Substances:
These include ammonia, urea, uric acid, creatine, creatinine, etc.
7. Dissolved Gases:
Water of blood plasma contains oxygen, carbon dioxide and nitrogen in dissolved form.
8. Anticoagulant:
Blood plasma contains a conjugated polysaccharide, the heparin which prevents coagulation of blood inside blood vessels.
9. Hormones:
These are secreted and released in blood by endocrine glands.
10. Vitamins and Enzymes:
Different kinds of vitamins and enzymes are present in the blood plasma.
Functions of Blood Plasma:
These can be summarised as under:
(i) Transport,
(ii) Retention of fluid in blood,
(iii) Maintenance of blood pH,
(iv) Body immunity,
(v) Prevention of blood loss,
(vi) Conducting heat to skin for dissipation and
(vii) Uniform distribution of heat all over the body.
(B) Formed Elements (Blood Corpuscles):
Formed elements or blood corpuscles are of the following three types: Erythrocytes, Leucocytes and Thrombocytes.
(a) Erythrocytes (Red Blood Corpuscles or RBCs):
They are the most abundant cells in the human body.
Size:
Human RBCs are smaller than the white blood corpuscles. They are 7-8 pm in diameter.
Shape:
In fishes, amphibians, reptiles and birds RBCs are usually nucleated, oval and biconvex. But in mammals they are not nucleated, biconcave and circular. Only Camel and lama possess oval RBCs. Mature RBCs are without cell organelles such as nucleus, mitochondria and ER.
Number:
The total number of RBCs per microlitre (lµ l = 1 mm3 = 10-6 l) of blood is termed as the total count of RBCs. A normal adult man and woman have 5 and 4.5 million RBCs per cubic millimetre of blood respectively. Thus the total count of RBCs is more in man than in a woman.
It is due to the fact that women undergo menstruation. Less amount of haemoglobin leads to anaemia. Anaemia may be caused by loss of blood (haemorrhage), destruction of RBCs (haemolysis or faulty formation of blood).
The increase in number of RBCs may be during muscular exercise to meet the increased demand of oxygen and at high altitudes to cope with the low oxygen content of the air. An abnormal rise in RBC count is called polycythemia.
Decrease in the number of RBCs is called erythrocytopenia which causes oxygen shortage in the blood and tissues. It is important to note that the oxygen shortage stimulates the kidney cells to secrete a hormone named erythropoietin, into the blood. Erythropoietin stimulates the bone marrow to increase the production of RBCs.
Formation:
Formation of erythrocytes is called erythropoiesis. In the early few weeks of embryonic life, primitive nucleated RBCs are produced in the yolk sac. (One of the embryonic membranes).
In later embryonic stage, RBCs are mainly produced by the liver and spleen. But from birth onwards, RBCs are produced by bone marrow (throughout life). Hemocytoblasts in red bone marrow give rise to mature RBCs. Iron and proteins are necessary raw materials for the synthesis of haemoglobin.
However, vitamin В12 and folic acid stimulate the maturation of RBCs. Thus iron, protein, vitamin B12 and folic acid are essential for the formation of haemoglobin and RBCs. Deficiency of any of these nutrients can cause anaemia. Excess RBCs are stored in the spleen.

Life Span:
The life of a RBC is about 120 days.
Haemoglobin:
Haemoglobin is a conjugated protein. It comprises a basic protein globin joined to a non protein group heme, hence the name haemoglobin is given. A mammalian haemoglobin molecule is a complex of 4 heme molecules joined with 4 globin molecules. Heme is an iron-prophyrin ring. 100 ml of blood contains about 15 mg of haemoglobin. Haemoglobin is less in women due to menstruation.
Functions of RBCs:
(i) Transport of O2:
Haemoglobin of RBCs readily combines with oxygen to form oxyhaemoglobin. In the tissues oxyhaemoglobin readily gives up its oxygen. This oxygen is used for oxidation of food.
(ii) Transport of СO2:
RBCs also participate in transporting carbon dioxide from tissues to lungs. Carbon dioxide combines with potassium carbonate of the red blood corpuscles to form potassium bicarbonate in the presence of an enzyme carbonic anhydrase. Carbon dioxide also combines with the amino group (—NH2) of the haemoglobin of red blood corpuscles to form carb-amino-haemoglobin.
(iii) Maintenance of pH of blood:
Moreover, the haemoglobin is an excellent acid base buffer which is largely responsible for maintaining the pH of blood. Acidity of blood results haemoglobin to carry less oxygen.

(b) Leucocytes (White Blood Corpuscles or WBCs):
Leucocytes do not have haemoglobin.
Number:
The number of leucocytes per micro-litre of blood is called the total leucocyte count (TLC). This varies from 4-11 x 103/cu mm of blood in humans. Thus, they are less in number than the RBCs. Rise in WBC count is termed leucocytosis. Increased TLC shows that there is acute bacterial infection. Abnormal increase of WBCs is in malignancies like leukemia (blood cancer).
Fall in WBC count is called leukopenia. In some conditions, such as folic acid deficiency, the total count of WBC decreases. The total count of WBC is useful in diagnosing various diseases. Normal or low TLC is in viral infection, malaria, typhoid or tuberculosis. Differential Leucocyte Count (DLC) means detecting the number of different kinds of leucocytes.
Normal DLC (Adults):

Shape:
The leucocytes are rounded or irregular in shape. They can change their shape like Amoeba and are thus, capable of amoeboid movement. This enables them to squeeze out of blood capillaries into the tissues (extra vascular regions). This process is called diapedesis.
Size:
The WBCs are larger than the RBCs. Their size is from 12 to 20 µm.
Colour:
The WBCs are colourless.
Structure:
A leucocyte consists of cell membrane, nucleus and cytoplasm. The cytoplasm contains mitochondria, Golgi apparatus, centrioles besides other cell organelles.
Types:
The leucocytes are of two main types: Agranulocytes and granulocytes.
Agranulocytes:
The granules are not found in the cytoplasm of these cells.
The agranulocytes are of two types:
(i) Lymphocytes:
They are smaller in size containing scant cytoplasm with large rounded nucleus. They are non-motile and non-phagocytic. They produce antibodies to destroy microbes and their toxins reject grafts and kill tumour cells. They also help in healing of injuries. Lymphocytes exist in two major groups in circulation. These are B- and T-lymphocytes.
(ii) Monocytes:
They are the largest of all types of leucocytes and somewhat amoeboid in shape. They have much cytoplasm. The nucleus is bean-shaped. They are motile and phagocytic in nature and engulf bacteria and cellular debris. Generally they change into macrophages after entering tissue spaces.
Granulocytes:
They contain granules in their cytoplasm. Their nucleus is irregular or lobed or subdivided. According to their staining property, the granulocytes are divided into three types.
(i) Eosinophil’s:
The nucleus is two lobed. They have coarse granules. Their granules take acidic stains (e.g., eosin). Their number increases in people with allergic conditions such as asthma or hay fever. They also help in dissolving blood clot. They are nonphagocytic. They seem to play a part in the immune system.
They have some similarity to lysosomes. Eosinophil’s can attach themselves to parasitic forms and cause their destruction by liberating lysosomal enzymes on their surface. Cytoplasm contains abundant coarse granules which pick acidic stain like eosine. They are, therefore, also called acidophils. The increase in number of acidophils during allergy is called eosinophilia.
(ii) Basophils:
The nucleus is usually three lobed. They have less number of coarse granules. Their granules take basic stain (e.g., methylene blue) strongly. Both mast cells and basophils liberate histamine, heparin as well as smaller quantities of bradykinin and serotonin. They are probably like mast cells of connective tissue.
(iii) Neutrophils:
The nucleus is many lobed. They have fine granules. They stain weakly with both acid and basic stains. Neutrophils are the most numerous of all leucocytes. Certain neutrophils in female mammals possess a small spherical lobe attached to their nucleus by a stalk.
This lobe is called drum stick (= sex chromatin) or Barr body. Barr is the name of the scientist. Drumstick is formed by transformation of an X-chromosome. They eat harmful germs and are, therefore, phagocytic in nature.
Formation:
Formation of leucocytes is called leucocytosis or leucopoeisis. The granulocytes and monocytes are formed only in bone marrow. Lymphocytes are produced mainly in lymph nodes, spleen, thymus, tonsils, bone marrow and Peyer’s patches of small intestine.
Life Span:
The life of the granulocytes once released from the bone marrow is normally 4 to 8 hours circulating in the blood and another 4 to 5 days in the tissues. The monocytes also have a short life span of 10 to 20 hours. The lymphocytes have life spans of few days or months or even years, but this depends on the body’s need for these cells.
Ratio of RBCs to WBCs is 700:1.
(C) Thrombocytes (= Blood platelets):
In mammals thrombocytes are called blood platelets.
Number:
They are fewer than the RBCs and more than the WBCs in number. There are about 250,000 platelets in a cubic millimetre of blood. Increase and decrease in the number of platelets is known as thrombocytosis and thrombocytopenia respectively.
Shape:
Blood platelets are really cell fragments rather than true cells. They are rounded or oval disc like bodies.
Size:
Platelets are 2-3 micro-meters in diameter. Thus they are much smaller than both the red and white blood corpuscles.
Colour:
Platelets are colourless.
Structure:
They are flat and non-nucleated fragments of the cells. They are simply bits of protoplasm, bounded by a membrane and contain a few cell organelles and secretory granules in the cytoplasm. They have a group of basophilic granules in the centre which give the appearance of a nucleus.
Formation:
Platelets are formed from the megakaryocytes (very large cells of the bone marrow). Formation of thrombocytes is called thrombopoiesis.
Life span:
Normal life span of blood platelets is about a week.
Function:
When an injury is caused, the blood platelets release certain chemicals which are called the platelet factors (e.g., thromboplastin). The platelet factors help in the clotting of blood.
Haemopoiesis:
The process of formation of blood is called haemopoiesis and the tissues which form blood corpuscles are termed the haemopoietic tissues. In frog, spleen, liver and lymph nodes are main sites of haemopoiesis. During rains haemopoiesis also occurs in bone marrow due to an active life of frog. In tadpoles kidneys are also haemopoietic.
In mammals, yolk sac (an embryonic membrane), liver, bone marrow, lymph nodes, spleen and thymus are the heomopoietic organs in the embryo. In adults most of the blood corpuscles are formed in the red bone marrow of long bones. Lymphocytes are, however, formed in thymus, some in spleen, lymph nodes, tonsils and Peyer’s patches.
Table: Summary of Human Blood Corpuscles

Functions of Blood:
On the basis of the above description, the general functions of blood are:
(1) Transport of Food Materials.
(2) Transport of Respiratory Gases.
(3) Transport of Hormones.
(4) Transport of Excretory Matter.
(5) Transport of Heat.
(6) Defence against Infection.
(7) Temperature Regulation.
(8) Water Balance.
(9) Maintenance of pH.
(10) Prevention of Excessive Loss of Blood.
(11) Helps in Healing.
(12) Maintenance of Physiological Cooperation.
II. Lymph:
Definition:
Lymph is a mobile connective tissue comprising lymph plasma (fluid) and lymph corpuscles (cells).
Composition (A) Lymph Plasma:
It is similar to that of blood but has fewer blood proteins, less calcium and phosphorus and high glucose concentration. Mainly globulin proteins are present which are actually antibodies. Other components of the lymph plasma are very much like that of blood plasma, i.e., organic, inorganic substances, water, etc.
(B) Lymph Corpuscles:
These are floating amoeboid cells, the leucocytes (white blood corpuscles), which are mostly lymphocytes. Erythrocytes (red blood corpuscles) and platelets are absent in lymph.
Lymphoid Organs:
The organs which secrete lymph are called lymphoid organs. Besides the lymph nodes, tonsils, thymus gland, spleen and Peyer’s patches are the other lymphoidal organs. Liver also produces lymph. The spleen is a large lymphatic organ in the body.
Functions of Lymph:
1. Lymph acts as a “middle man” which transports oxygen, food materials, hormones, etc., to the body cells and brings carbon dioxide and other metabolic wastes from the body cells to blood and then finally pours the same into the venous system.
2. Body cells are kept moist by the lymph.
3. Lymph nodes produce lymphocytes. Lymph takes lymphocytes and antibodies from the lymph nodes to the blood.
4. It destroys the invading microorganisms and foreign particles in the lymph nodes.
5. It absorbs and transports fat and fat soluble vitamins from the intestine. Lymphatic capillaries present in the intestinal villi are called lacteals which are associated with absorption and transportation of fat and fat soluble vitamins.
6. It brings plasma protein macromolecules synthesized in the liver cells and hormones produced in the endocrine glands to the blood. These molecules cannot pass into the narrow blood capillaries but can diffuse into the lymphatic capillaries.
7. Lymph maintains the volume of the blood. As soon as the volume of the blood reduces in the blood vascular system, the lymph rushes from the lymphatic system to the blood vascular system.
(C) Reticular Connective Tissue:
Structure:
This tissue consists of star-shaped reticular cells whose protoplasmic processes join to form a cellular network. The reticular fibres are present on the reticular cells. They are composed of a protein called reticulin. Matrix and some other cells such as macrophages, lymphocytes and adipose cells are also present (Fig. 7.28)
Location:
Reticular connective tissue is present in the liver, spleen, lymph nodes, thymus, tonsils, bone marrow and lamina propria of the gut wall.
Functions:
The reticular connective tissue is especially adapted to provide strength and support as it forms the supporting framework (stroma) of many organs. It also helps to bind together the cells of smooth muscles. The reticular cells are phagocytic and form defence mechanism of the body.

(D) Pigmented Connective Tissue:
Structure:
The cells are irregular in shape and are called pigment cells (= chromatophores or melanophores; Fig. 7.29) which contain yellowish brown, black or blue melanin pigment granules. Melanin is in fact, produced by other cells called melanocytes. Chromatophores simply phagocytise the melanin from melanocytes like macrophages.
Location:
Pigmented connective tissue is present in the choroid, ciliary body and iris of the eye and dermis of the human skin.
Functions:
The pigmented connective tissue gives colour to the structures.

(E) Mucoid Connective Tissue:
In addition to above mentioned connective tissues, mucoid tissue occurs as a foetal or embryonic connective tissue. It is present in the umbilical cord. The most conspicuous component of the mucoid tissue is a jelly like substance, called whartson’s jelly.
Some delicate collagen fibres and primitive type of fibroblasts arc also present. Mucoid tissue (mucous connective tissue) also occurs in vitreous humour of the eye and in comb of cock.
No comments:
Post a Comment